Insulin costs have skyrocketed, meaning that more and more patients are unable to afford analogue preparations and must return to the bad old days of using human insulins in a vial rather than preloaded pens. While there are definitely downsides to the switch, at least one study conducted in a Medicare population provides reassurance to clinicians and patients that the switch can be done without a loss of control.
What are the basic steps in switching a patient from an analogue insulin to a split mixed human insulin regimen? Dr Jay Shubrook walks us through the math.

First, calculate the total daily dose.
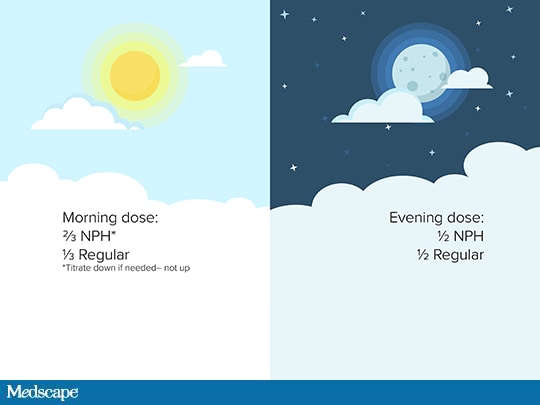
Divide the daily dose by 3. Give two thirds of the total dose in the morning (two thirds as intermediate-acting and one third as short-acting), ideally before breakfast. Give one third in the evening (one half as intermediate-acting and one half as short-acting), ideally before dinner.
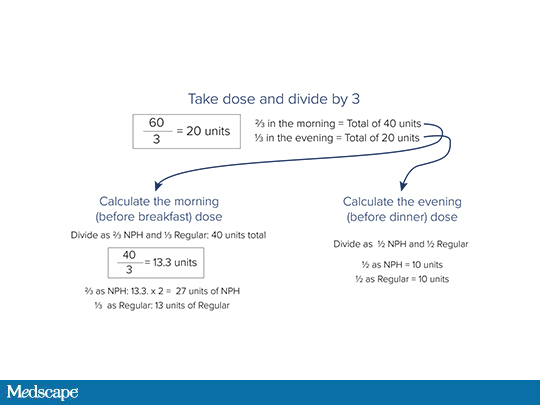
Let's use the example of a patient who had been receiving a total daily insulin dose of 60 units. That would be calculated as 40 units pre-breakfast (27 units NPH, an intermediate-acting insulin; and 13 units regular) and 20 units pre-dinner (10 units NPH and 10 units regular).
Follow Medscape on Facebook, Twitter, Instagram, and YouTube
Medscape Family Medicine © 2019 WebMD, LLC
Any views expressed above are the author's own and do not necessarily reflect the views of WebMD or Medscape.
Cite this: Doing the Math: Converting Analogue to Human Insulin - Medscape - Jun 12, 2019.











Comments